Monitoring for colorectal cancer recurrence

Why recurrence testing matters
After treatment ends, the path continues. Monitoring for recurrence, also called surveillance, is essential to detect cancer early if it returns. Early detection improves the chances of successful intervention and empowers survivors to stay proactive in their care.
When you see your medical provider, they may use several different tools to assess:
- How well you are responding to treatment (if you are currently in treatment)
- If further treatment or a change may be needed
- Whether there are signs that the cancer has spread, returned, or progressed
Surveillance strategies aimed at early detection increase the chance that cancer can be treated and cured. New tools are available to detect traces of cancer in the blood.
The odds for cancer recurrence are higher if the initial tumor was diagnosed at an advanced stage.

What Is cancer recurrence?
Recurrence means the cancer has returned after a period of remission. It may appear:
- Locally: in the same area as the original tumor
- Regionally: in nearby lymph nodes or tissues
- Distantly: in other organs like the liver, lungs, or brain
With colorectal cancer, you may not have symptoms at all, or your recurrence symptoms may be the same as your original symptoms, such as abdominal pain, bloody stools, weight loss, diarrhea, or constipation.
A colonoscopy may also reveal a recurrence, which is why it’s important to stay on schedule with your screening tests and other follow-up appointments. The sooner a recurrence is diagnosed, the better the chances are for survival.

Cancer monitoring recommendations
Now that you have completed your treatment — whether your treatment plan included surgery, chemotherapy, and/or radiation — you and your medical team should discuss your follow-up care plan. The plan will include ongoing monitoring and should also address lifestyle and emotional needs.
- Talk with your doctor (oncologist) about your risk of cancer coming back (recurrence) and how it affects your follow-up care plan and testing schedule.
- Keep your scheduled follow-up visits. These visits are important. While you cannot guarantee that cancer will not come back, routine visits will increase your chance of catching a recurrence earlier, making it easier to treat.
- Ask your care team about new tests that may be available for early detection of recurrence. There are many new non-invasive technologies (e.g., blood tests) that make it easier and faster to find cancer when it recurs.
- Find out if you can go to a survivorship and wellness clinic for your follow-up visits. While many survivors get follow-up care with their oncologist or with their primary care doctor, these clinics have specialized experts who can also help with nutrition, physical activity, and other health needs.
- Talk to your medical team about your fears and anxiety. Some patients feel lonely after the frequent visits they are used to with the care team added. Our cancer care clinical navigators are available anytime to talk through your concerns.
Comparison of cancer monitoring methods
Colorectal Cancer Recurrence Testing Comparison Chart
Test Type | Purpose / Use Case | Sample Type | Frequency / Timing | Key Advantages | Limitations / Notes |
Clinical Surveillance | Symptom review, physical exam | In-person visit | Every 3–6 months (first 2–3 years) | Non-invasive, holistic assessment | May miss asymptomatic recurrence |
Colonoscopy | Detect local recurrence or new polyps | Visual exam | Every 1–3 years | Gold standard for local detection | Requires prep and sedation |
CEA Blood Test | Tumor marker monitoring | Blood | Every 3–6 months (first 3 years) | Widely available, low cost | Not reliable for all patients |
CT Scan | Detect metastases or local recurrence | Imaging | Every 6–12 months | High-resolution internal imaging | Radiation exposure; may miss small lesions |
MRI / PET Scan | Detailed imaging for specific cases | Imaging | As needed | Useful for soft tissue or metabolic data | Higher cost; limited availability |
ctDNA Testing (e.g., Signatera) | Detect minimal residual disease (MRD), predict recurrence | Blood | Post-surgery, then every few months | Highly sensitive, sometimes personalized | Not FDA-approved for recurrence; CLIA-certified |
CTC Testing (e.g., CellSearch) | Monitor progression, recurrence, treatment response | Blood | Serial testing during remission | Real-time insights; FDA-cleared for mCRC | Less common in early-stage CRC |
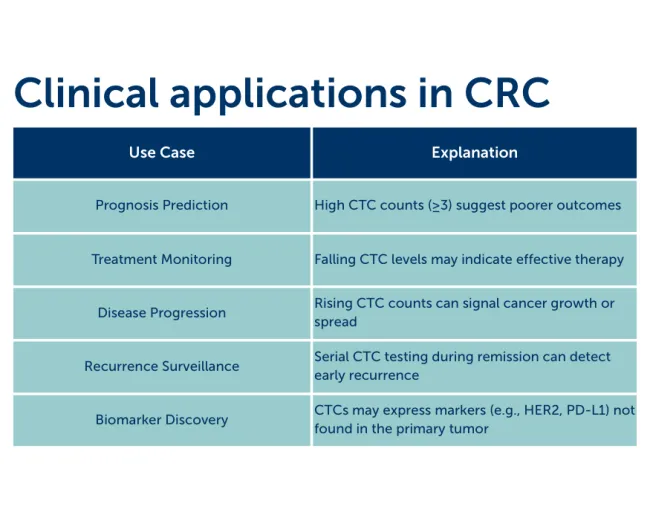
What is CTC biomarker testing?
Circulating Tumor Cell (CTC) testing is a liquid biopsy technique that detects whole cancer cells shed from a tumor into the bloodstream. These cells can travel to other parts of the body and potentially form new tumors.
How It Works
- A blood sample is drawn and sent to a lab
- Specialized techniques isolate and count CTCs per 7.5 mL of blood
- The most widely used test is CellSearch, FDA-cleared for metastatic breast, prostate, and colorectal cancers
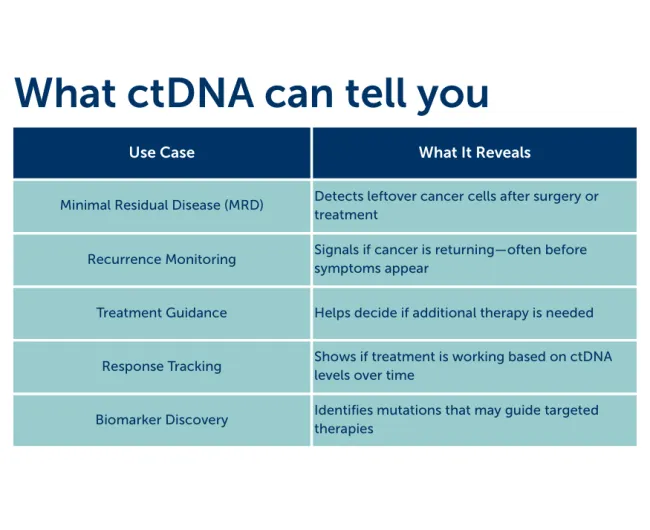
What is ctDNA testing?
Circulating tumor DNA (ctDNA) testing is a type of liquid biopsy that looks for tiny fragments of DNA shed by cancer cells into the bloodstream. These fragments can reveal whether cancer is still present after treatment—or if it might be coming back.
How It Works
- When cancer cells die, they release bits of their DNA into your blood
- A blood sample is drawn and sent to a lab
- Advanced technologies (like next-generation sequencing) scan for tumor-specific mutations or methylation patterns
- Some tests are tumor-informed, meaning they’re customized to your unique cancer profile
- Others are tumor-agnostic, looking for general cancer-linked markers
How is ctDNA used?
After completing treatment
- ctDNA testing is an option for survivors who have finished curative treatment and are stage II or stage III. Along with CEA, ctDNA is currently approved for monitoring disease recurrence in survivors of stage II and III colorectal cancer. Additional tests such as CT, MRI, or PET scans may be necessary to locate the cancer recurrence.
After surgery
ctDNA can also be used to monitor any residual (leftover) cancer after surgery in low-risk stage II and III colon cancer and stage IIA rectal cancer. This can determine if adjuvant (after surgery) chemotherapy is needed in low-risk patients. Chemotherapy is the standard of care for high-risk, more advanced colon cancer and high-risk rectal cancer, which includes radiation with or without chemotherapy.
CTC vs. ctDNA Testing
Feature | CTC Testing | ctDNA Testing |
Target | Whole cancer cells | DNA fragments from dying cancer cells |
Sample Type | Blood | Blood |
Use Cases | Prognosis, progression, recurrence | MRD detection, mutation tracking |
FDA Approval | CellSearch® for metastatic cancers | Varies by test; some are CLIA-certified |
CTC testing is especially valuable in metastatic CRC, offering real-time insights into disease status and treatment efficacy

Can a recurrence be treated?
Treatment for recurrent colorectal cancer is based on many things, including:
- Location of the cancer
- Other health issues
- Individual preferences
The main treatments used are surgery, chemotherapy, radiation, or a combination of any of these. Other treatments, such as liver directed therapy or immunotherapy, may be recommended.
Joining a clinical trial may also be an option, where you may have access to more recently developed treatments and experimental medications.
Talk to your care team about clinical trials that are appropriate for you.
ctDNA Testing Options
How it’s done:
A small blood sample (about a teaspoon) is taken — usually during a routine visit. The lab separates the plasma (the liquid part of your blood) and looks for tiny clues that cancer might be coming back. These clues can include tumor DNA fragments floating in your blood or whole cancer cells that may have broken off from a tumor.
One common method used in practice is RT-PCR, a fast and affordable test that uses light-sensitive probes to detect genetic changes. It’s widely used and helps doctors track whether cancer-related DNA is present in your blood.
FDA-approved and emerging options:
FoundationOne Tracker (Foundation Medicine)
CLIA-certified, laboratory-developed test (LDT), and typically used after surgery or systemic therapy to provide real-time insights into disease status, often before changes appear on imaging. FoundationOne Tracker is a customized blood-based assay from Foundation Medicine that uses a patient’s unique tumor profile to monitor molecular residual disease (MRD) in individuals with solid tumors.
This option analyzes circulating tumor DNA (ctDNA) based on a patient’s unique tumor profile, enabling clinicians to track treatment response, detect early signs of recurrence, and make more informed decisions about ongoing cancer management.
Signatera (Natera)
CLIA-certified; granted FDA Breakthrough Device designation for minimal residual disease (MRD) detection in CRC. High sensitivity (~88%) and specificity (~95%). It uses a tumor-informed approach, meaning the test is customized to each patient’s unique cancer mutations for highly sensitive tracking.
It’s commonly used in stage II–III colorectal cancer to help guide decisions about adjuvant therapy and long-term surveillance. The test is backed by strong clinical evidence from studies like DYNAMIC and CIRCULATE, and is increasingly adopted in oncology practices across the U.S.
Oncodetect MRD (Exact Sciences)
A molecular residual disease (MRD) test designed to detect colorectal cancer (CRC) recurrence earlier and more precisely than traditional imaging. Oncodetect uses whole-exome sequencing to track up to 200 tumor-specific variants. It can detect a single ctDNA molecule among 20,000 cell-free DNA molecules.
Oncodetect is currently under review by the U.S. Food and Drug Administration (FDA) for its use as an MRD test. While it has not received full FDA approval, it has achieved a major milestone: Medicare coverage through CMS’s MolDX program for serial use in patients with stage II, III, and resectable stage IV colorectal cancer.
Guardant Reveal (Guardant Health)
Blood-based, tissue-free test developed by Guardant Health for molecular residual disease (MRD) detection and recurrence monitoring in patients with early-stage solid tumors, particularly colorectal and breast cancers. Guardant Reveal has a strong performance (91% serial sensitivity, ~98% specificity, average lead time ~4 months before imaging). This test method is not yet FDA-cleared.
Analyzing circulating tumor DNA (ctDNA) and epigenomic signals directly from plasma, it enables clinicians to assess treatment response and detect minimal residual disease without requiring tumor tissue. Guardant Reveal is a laboratory-developed test (LDT) and offers a convenient, noninvasive option for ongoing cancer surveillance.
Haystack MRD (Haystack Oncology/Quest Diagnostics)
Receiving FDA Breakthrough Device Designation in August 2025, this cutting-edge, blood-based tool is designed to detect minimal residual disease (MRD) in patients with stage II colorectal cancer after surgery. It’s part of a growing movement toward precision oncology.
COLVERA (CSIRO)
A CLIA-certified, laboratory-developed test, is a doctor-ordered blood test that detects colorectal cancer–linked DNA fragments in the bloodstream, helping identify possible recurrence or residual disease alongside CEA testing.
Comparison snapshot
Test Name | FDA Status | Approach | Primary Use Case | Notes |
Signatera | CLIA-certified; breakthrough | Tumor-informed | MRD detection, recurrence tracking | Widely used in oncology clinics |
Haystack MRD | FDA Breakthrough Device Designation | Tumor-informed | MRD in stage II CRC | High sensitivity; expanding trials |
FoundationOne Tracker | CLIA-certified; breakthrough | Tumor-informed | MRD, recurrence, treatment response | Emerging in solid tumor surveillance |
Guardant Reveal | Not FDA-approved; developed as a CLIA-certified Laboratory Developed Test (LDT) | Tumor-agnostic, tissue-free ctDNA assay using epigenomic and genomic signals | MRD, recurrence in early-stage colorectal cancer | Covered by Medicare for stage II–III CRC if initiated within 3 months post-treatment; does not require tumor tissue; complements standard follow-up tools like colonoscopy, CEA, and imaging |
OncoDetect | Not FDA-approved; developed as a CLIA-certified Laboratory Developed Test (LDT) | Tumor-informed ctDNA | MRD monitoring in patients with solid tumors | Medicare coverage through CMS’s MolDX program for serial use in patients with stage II, III, and resectable stage IV colorectal cancer; Typically used after surgery or chemotherapy to monitor for relapse. |
CTC testing options
How it’s done:
CTC testing looks for whole cancer cells that may have broken away from a tumor and entered your bloodstream. A small blood sample (about a teaspoon) is taken. The lab uses a specialized process to find and count cancer cells in the blood. These cells are identified based on their size and unique features that separate them from normal blood cells.
The most commonly used test, called CellSearch, is FDA-cleared and used for metastatic colorectal cancer. If five or more cancer cells are found in the sample, the test is considered positive, which may suggest that the cancer is active or progressing.
FDA-approved and emerging options:
CellSearch (Menarini Silicon Biosystems)
First and only FDA-cleared system for the detection and enumeration of circulating tumor cells (CTCs) in whole blood, developed by Menarini Silicon Biosystems.
It uses immunomagnetic separation and fluorescence imaging to isolate and identify CTCs based on epithelial cell markers, making it a powerful tool for prognostic assessment, treatment monitoring, and clinical research in metastatic cancers such as breast, prostate, and colorectal. CellSearch provides standardized, reproducible results and has been widely validated in clinical studies, establishing it as a benchmark in CTC-based liquid biopsy technologies.
Parsortix (ANGLE)
Cell-based liquid biopsy system developed by ANGLE plc that captures and harvests circulating tumor cells (CTCs) from blood samples for downstream analysis.
Unlike traditional ctDNA tests, Parsortix isolates intact cancer cells using a patented microfluidic cassette that separates them based on size and deformability—without relying on surface markers. This enables noninvasive cancer detection, treatment response monitoring, and biomarker discovery. Parsortix is an emerging option in colorectal cancer that could offer a unique platform for precision oncology and translational research.
ClearCell FX
An automated, label-free microfluidic system for enriching circulating tumor cells (CTCs) from blood, using Dean Flow Fractionation (DFF) to separate cells based on mechanical properties like size and deformability, preserving cell viability for downstream analysis and functional studies.
Designed for noninvasive cancer diagnostics and monitoring, ClearCell FX is an emerging option that enriches CTCs based on their physical properties—such as size and deformability—without relying on surface markers, enabling downstream molecular analysis.
Comparison snapshot
| Platform | FDA Status | Use Case in CRC | Notes |
| CellSearch | FDA-cleared | Prognosis, recurrence, mCRC | Most validated; limited to EpCAM+ CTCs |
| Parsortix | Emerging | Research, early detection | Label-free; size-based isolation |
| ClearCell FX | Emerging | Research, metastatic profiling | Microfluidic-based; high purity |
| CTC + RNAseq | Experimental | Biomarker discovery, treatment | May guide immunotherapy decisions |
CEA testing options
How it’s done:
CEA (carcinoembryonic antigen) is a protein that can show up in higher amounts if colorectal cancer returns. Doctors use it as a common blood test to help monitor for recurrence after treatment.
A small blood sample (about a teaspoon) is taken — usually during a routine visit. The sample is sent to a lab, where technicians measure the amount of CEA in your bloodstream. If your CEA level is rising over time, it may be a sign that cancer has come back or is growing.
Doctors use this test regularly after treatment because it’s a helpful early warning tool. In fact, about 60–90% of people whose colorectal cancer returns will show elevated CEA levels. If your results are higher than expected, your care team may order follow-up tests — like a CT scan, PET scan, or colonoscopy — to look for signs of recurrence.
FDA-approved and emerging options:
There is no specific FDA clearance for CEA as a recurrence test. While traditional CEA testing is well-established, newer platforms aim to improve sensitivity, accuracy, and integration with other biomarkers.
Standard CEA Blood Test
CEA testing has been a standard part of colorectal cancer follow-up care for decades. While individual test kits may vary, the overall method — measuring CEA levels in blood — is widely FDA-cleared and routinely used in clinical practice. These tests are typically recommended every 3 to 6 months during the first two years after surgery, and then every 6 months for up to five years.
They’re affordable, easy to access through most hospitals and diagnostic labs, and backed by national guidelines from organizations like NCCN and ASCO. For many patients, CEA testing is a routine and reassuring part of follow-up care.
Advanced Immunoassays
Advanced CEA testing methods, such as chemiluminescent microparticle immunoassays (CMIA) and electrochemiluminescence (ECL), are designed to improve lab efficiency and accuracy.
These technologies offer faster turnaround times and more consistent results compared to traditional methods, making them ideal for high-volume diagnostic settings. Their streamlined performance supports automated lab workflows, helping ensure timely and reliable monitoring for patients undergoing colorectal cancer surveillance.
Mass Spectrometry–Based CEA Detection
Some emerging methods for CEA testing are still in the research and early clinical stages, but they show promise for improving accuracy — especially in complex cases. These advanced techniques offer higher specificity, meaning they’re better at detecting true cancer signals without being affected by other proteins in the blood. In the future, they may be especially useful when used alongside other biomarkers in multi-marker panels, helping doctors get a clearer picture of recurrence risk and treatment response.
AI-Integrated Platforms
Some experimental approaches to recurrence monitoring are exploring how to combine CEA levels with other biomarkers and clinical information to better predict a patient’s risk of cancer coming back. These strategies use advanced data analysis, sometimes powered by artificial intelligence, to create a more personalized surveillance plan based on your unique health profile.
While still in development, this kind of testing could one day help doctors tailor follow-up care more precisely, reducing unnecessary procedures and catching recurrence earlier.
Comparison snapshot
Platform Type | FDA Status | Use Case | Notes |
Standard CEA Blood Test | FDA-cleared | Routine recurrence monitoring | Widely used; guideline-supported |
Advanced Immunoassays | FDA-cleared | Lab automation, improved accuracy | Used in high-throughput labs |
Mass Spectrometry Platforms | Emerging | Enhanced specificity | Research phase; not yet standard practice |
AI-Integrated Surveillance | Experimental | Predictive modeling | Promising for future personalized care |
CEA remains a cornerstone of colorectal cancer follow-up, but pairing it with ctDNA, imaging, and clinical review offers a more complete picture.

Strategic considerations
Surveillance plans are tailored by oncologists based on:
- Cancer stage
- Treatment history
- Risk factors
- Patient preferences
Plans may evolve over time, incorporating new technologies like ctDNA and CTC testing to enhance precision and personalization.
Questions to ask your doctor
After you have finished treatment, you may have a number of questions swirling in your mind. Here are some questions to consider asking your healthcare team to make sure you are clear on your next steps.
Follow-up schedule for colorectal cancer survivors
For a colorectal cancer patient, recurrence testing typically begins shortly after completion of initial treatment, such as surgery or chemotherapy. Blood-based molecular residual disease (MRD) tests—like ctDNA assays—are often performed every 3 to 6 months during the first two years, when the risk of recurrence is highest. This schedule may be paired with periodic imaging and clinical evaluations. If no ctDNA is detected, testing intervals may be extended; however, if ctDNA is found, more frequent monitoring or therapeutic intervention may be recommended. The exact schedule is tailored to the patient’s cancer stage, treatment response, and overall risk profile.
Years 0–2 (Immediately After Treatment)
Frequency: Every 3–6 months
Includes:
- Physical exam & symptom review
- CEA blood test (if applicable)
- ctDNA testing (e.g., Signatera, Haystack MRD) for stage II–III patients
- CT scan of chest, abdomen, and pelvis every 6–12 months
- Colonoscopy at 1 year post-surgery (or sooner if not done before)
Goal: Detect early recurrence, guide adjuvant therapy decisions, and monitor residual disease.
Years 3–5
Frequency: Every 6 months
Includes:
- Physical exam & symptom review
- CEA blood test
- ctDNA testing (if previously used)
- CT scan annually or as clinically indicated
- Colonoscopy every 3–5 years based on findings and risk level
Goal: Continue surveillance for recurrence and manage long-term side effects.

Beyond Year 5
Frequency: Annually or as needed
Includes:
- Physical exam & symptom review
- Colonoscopy per gastroenterologist’s recommendation
- Imaging or blood tests only if symptoms or prior history suggest recurrence risk
Goal: Transition to survivorship care, focusing on wellness, lifestyle, and emotional support.

Coping with a cancer recurrence
Colorectal cancer recurrence can bring back many of the difficult emotions you felt when you were originally diagnosed.
This time around, however, can be different because:
- You are better prepared and know much more about colorectal cancer than the first time you faced it.
- You know which coping strategies work for you, such as physical activity, spending time with friends and family, and meditation.
- You have a care team that you know — you are going back to familiar faces and people who know you.
- New treatments are rapidly becoming available.
CRCtalks: The Survivor's Toolbox
Jennifer R. Klemp, PhD, MPH, MA, of The University of Kansas Cancer Center, discusses strategies and resources you can use to protect your health and well-being in survivorship. Dr. Klemp discusses topics including recurrence monitoring, germline testing, and self-care.
Educational content developed with support from
Get the recurrence download
PDFTop resources

Alliance Breaks Down New ACS Screening Guidelines
The Colorectal Cancer Alliance is urging Americans to prioritize colorectal cancer screening, as the American Cancer Society (ACS) released updated guidelines today.

A blood test that sees what scans can't
For many cancer patients, the end of active treatment brings a new kind of dread. Scans every few months and anxious waits for results. A blood test is changing that experience for a growing number of patients.

HAI therapy proves pivotal for pioneering patient
When Helen was diagnosed with metastatic colorectal cancer, the biggest concern for her medical team was that her cancer had spread to her liver. One type of therapy, hepatic artery infusion, offered a path forward, but there was a catch. Nobody at her hospital had ever done it before. She'd have to be first.